
Show all clinical related articles
Canine Benign Prostatic Disease - Part 2
Catriona Curtis BVM&S MRCVS - 24/11/2021
CANINE BENIGN PROSTATIC DISEASE -
Pathogenesis, Diagnosis and Treatment (Part 2)
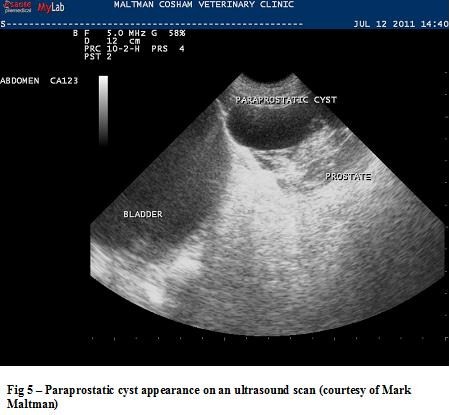
Prostatic Cysts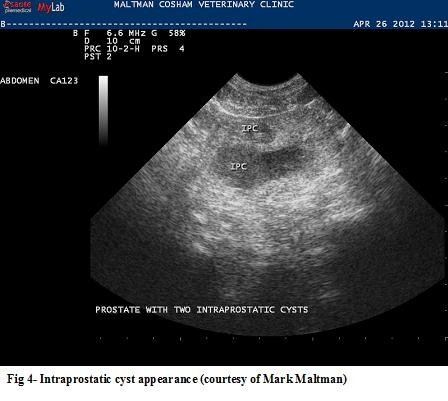
It is more common to find prostatic cysts in middle aged to older dogs. Clinical signs are similar to BPH but can also include abdominal pain, distension and anorexia and lethargy. On rectal palpation the prostate may feel enlarged and irregular. Urinalysis is similar to BPH.
Radiography may show prostatic displacement, in the presence of extra-prostatic cysts. Mineralisation of the cysts may also be seen. Contrast radiography can be used to evaluate if the cyst is para-prostatic or not.
Ultrasonography will provide a definitive diagnosis. It allows the size, type and location of the cysts to be diagnosed. The fluid in the cysts is usually hypoechoic or anechoic. Abscessation can occur secondary to prostatic cysts. The fluid in these cases will often be hyperechoic.
Intra-prostatic cysts will often regress with treatment for BPH. If treatment is medical it will need to be repeated at appropriate intervals. NSAIDs are often required. Surgery can be performed for extra-prostatic cysts. Large intra-prostatic cysts may also require surgery. It is advised that you consult a surgery text book for a description of the possible procedures and complications.
Prostatitis
Clinical signs of acute prostatitis can be severe. They will often include anorexia, pyrexia, stranguria, haematuria, abdominal pain, vomiting, malaise, constipation, obstipation and an unwillingness to breed. In severe cases the blood-prostate barrier may be breached and haematogenous spread can occur. This may result in sepsis, DIC or multi organ failure.
On rectal palpation the prostate is almost always painful, swollen and asymmetrical in enlargement. The degree of enlargement often depends on the cause of the prostatitis and if abscessation has occurred. There may be numerous haematological and biochemical changes. They can include pre or post renal azotemia, elevated ALT and ALKP, hypo-proteinaemia and electrolyte imbalances. There will usually be a leuocytosis and a neutrophillia, with a left shift. Urinalysis will often reveal pyuria and haematuria. Culture can help to identify the causative organisms. A prostatic wash will often reveal neutrophils and again culture will be positive.
Ultrasonography will demonstrate a focal to diffuse heterogeneous echogenicity. There are usually cavitating lesions present with hypoechoic fluid. Radiographs may demonstrate prostatic enlargement.
Treatment needs to include appropriate antibiosis and pain relief. It often needs to be very aggressive. Intravenous fluids are often required and electrolyte imbalances need to be addressed.
Antimicrobials are critical and choice should ideally be made on bacterial susceptibility and the pharmacokinetics of the antimicrobial. When the blood-prostate barrier has been breached antimicrobial penetration is good. However this is not always the case and penetration can be difficult. Erythromycin and trimethoprim penetrate well due to their higher pH and lipid solubility. Because of the zwitterion characteristics of fluoroquinolones they can also be an appropriate choice (Smith 2008).
Treatment should be continued for a minimum of 4 weeks. NSAIDs are often critical but it is important to address any renal compromise first. Concurrent BPH should always be treated. Severe prostatic abscesses may need surgical treatment.
Prostatic Neoplasia
Clinical signs of prostatic neoplasia can mimic prostatitis. It is important to remember the rarity of the disease in relation to other prostatic diseases. The average age for diagnosis is 10 years and neutered middle to large breed dogs are over represented (Le Roy and Northrup 2008).
Clinical signs may also include weight loss, hindlimb weakness, abdominal pain and pelvic pain. It is not uncommon to find some clinical signs associated with metastasis. Diagnosis includes rectal palpation, urinalysis, haematology and biochemistry, radiography, ultrasonography, FNA and biopsies. A definitive diagnosis can only be made with histological findings after an incisional biopsy (Nelson Couto 2003). It can be a common mistake to diagnosis prostatic neoplasia on clinical signs alone.
Treatment unfortunately is often unrewarding. As they can be so aggressive metastasis has often occurred by the time of diagnosis. Treatment options include surgery, chemotherapy and radiotherapy (Le Roy and Northrup 2008). A combination is often required. Dogs with prostatic carcinoma have been shown to have an increased survival time if treated with piroxicam or carprofen. If BPH is present then it is important to treat as it may provide some palliative relief. Consultation with a specialist oncologist is advised.
The author would like to thank Mark Maltman of Maltman and Cosham vets for kindly providing the images for this article.
CLICK HERE to read Part 1 of this article on anatomy, pathogenesis and BPH
This article was kindly provided by Virbac, makers of Ypozane. Ypozane contains Osaterone acetate for more information contact Virbac Animal Health on 01359 243243, Woopit Business Park, Windmill Avenue, Woolpit, Bury St Edmunds IP30 9UP. This article was first printed in Veterinary Practice Magazine.

![]()
References
Albouy M, Sanquer A, Maynard L, Eun HM. Efficacies of osaterone and delmadinone in the treatment of benign prostatic hyperplasia in dogs. Veterinary Record (2008) 163, 179-183
Atalan G, Barr FJ, Holt PE. Comparison of ultrasonographic and radiographic measurements of canine prostatic dimensions. VetRadiol Ultrasound 1999;40:408–12.
Bamberg-Thalen BL, Linde-Forsberg C. Treatment of canine benign prostatic hyperplasia with medroxyprogesterone acetate. J Am Anim Hosp Assoc 1993;29:221–6.
Black GM, Ling GV, Nyland TG, Baker T. Prevalence of prostatic cysts in adult, large-breed dogs. J Am Anim Hosp Assoc 1998;34:177–80.
Bryan JN, Keeler MR, Henry CJ, Bryan ME, Hahn AW,Caldwell CW. A population study of neutering status as a risk factor for canine prostate cancer. Prostate 2007;67:1174–81.
EMEA. Ypozane scientific discussion.
Evans HE, Christensen GC. The urogenital system. In: Miller’s anatomy of the dog. WB Saunders; 1993. p. 514–516.
Gloyna RE, Siiteri PK, Wilson JD. Dihydrotestosterone in prostatic hypertrophy. J Clin Invest 1970;49:1746–53.
Gobello C. Dopamine agonist, anti-progestins, anti-androgens, long-term-release GnRH agonists and anti-estrogens in canine reproduction: a review. Theriogenology 2006;66:1560–7.
Gobello C, Corrada Y. Noninfectious prostatic diseases in dogs. Compend Contin Educ Vet 2002;24:99–107.
Johnston SD, Root Kustritz MV, Olson PN. Disorders of the canine prostate. In: Canine and feline theriogenology. WB Saunders; 2001. p. 337–355.
Krawiec DR, Heflin D. Study of prostatic disease in dogs: 177 cases (1981–1986). J Am Vet Med Assoc 1992;200:1119–22.
Kutzler M, Yeager A. Prostatic diseases. In: Textbook of veterinary internal medicine. WB Saunders; 2005. p. 1809–1819.
LeRoy BE and Northrup N. Prostate cancer in dogs: Comparative and clinical aspects. The Veterinary Journal 2008; doi:10.1016/j.tvjl.2008.07.012
Ling GV, Branam JE, Ruby AL, Johnson DL. Canine prostatic fluid: techniques of collection, quantitative bacterial culture, and interpretation of results. J Am Vet Med Assoc 1983;183:201–6.
Memon MA. Common causes of male dog infertility. Theriogenology 2007;68:322–8.
Nelson RW, Couto CG. Small Animal Internal Medicine – Disorders of the prostate gland; WB Saunders 2003 p.927-932
O'Shea J.D. Studies on the canine prostate gland: Factors influencing its size and weight. J. Comp. Pathol. 1962 72: 321-331.
Parry N. The canine prostate gland Part 1 – non inflammatory diseases. UK Vet Vol 12 No 1 January 2007
Ruel Y, Barthez PY, Mailles A, Begon D. Ultrasonographic evaluation of the prostate in healthy intact dogs. Vet Radiology Ultrasound 1998;39:212–6.
Smith J. Canine prostatic disease: A review of anatomy,pathology, diagnosis, and treatment. Theriogenology 70 (2008) 375–383
White RAS. Prostatic surgery in the dog. Clin Tech Small Anim Pract 2000;15:46–51.
This article was first published on VetGrad.co.uk in 2017.

